In 2026, couples facing azoospermia often ask how far specialist sperm retrieval can actually go, especially when data show that first‑time micro‑TESE sperm retrieval rates can reach about 64.6%, while repeated attempts drop to around 28.8% in non‑obstructive azoospermia. We created this in‑depth guide so you can understand how TESA, PESA, and TESE fit into modern fertility treatment, and how they may be used alongside IVF and ICSI in real clinical practice.
Key Takeaways
| Question | Short Answer |
|---|---|
| What are TESA, PESA, and TESE in male fertility treatment? | They are surgical sperm retrieval techniques used when sperm are not present in the ejaculate, described in detail on our dedicated TESA / PESA / TESE sperm retrieval page. |
| When do clinics consider sperm retrieval procedures? | Usually in azoospermia or very low sperm counts, especially when couples are planning IVF or ICSI treatment. |
| How are retrieved sperm usually used? | Most often with Intracytoplasmic Sperm Injection (ICSI), where a single sperm is injected directly into each mature egg. |
| What if sperm retrieval is not possible or not successful? | Some couples discuss donor options such as sperm donation or donor embryo adoption, depending on their goals and situation. |
| Can sperm be stored once retrieved? | Many clinics offer freezing of sperm and embryos, as explained on our cryopreservation (sperm and embryo freezing) page. |
| Where do TESA, PESA, TESE sit in the wider IVF journey? | They are part of our broader IVF procedures and treatment pathway for couples with male‑factor infertility. |
| Are these techniques used alone or with other ART methods? | They form one component of modern assisted reproductive technology, often combined with IVF, ICSI, PGT, and other procedures. |
Understanding TESA, PESA, TESE: The Basics Of Sperm Retrieval In 2026
When semen analysis shows azoospermia, we often look beyond the ejaculate and focus on whether sperm can be obtained directly from the epididymis or testicles using TESA, PESA, or TESE. Each technique targets a different anatomical site and uses a different approach, so the choice depends on whether the problem is obstructive or non‑obstructive and on each patient’s medical background.
In 2026, these procedures are usually integrated into a complete assisted reproduction plan, rather than carried out in isolation. Our role is to explain what each method involves in practical terms, what the realistic goals are, and how it may link to IVF or ICSI in your treatment plan.
What TESA, PESA, and TESE Stand For
TESA stands for testicular sperm aspiration, which is a needle‑based aspiration technique directly from the testicular tissue. PESA stands for percutaneous epididymal sperm aspiration, usually considered when sperm production appears normal but a blockage prevents sperm from entering the ejaculate.
TESE means testicular sperm extraction and usually involves removing tiny tissue fragments from the testis. These fragments are examined in the lab to find sperm for use with IVF and especially ICSI.
Why These Techniques Exist
Many couples ask why we cannot simply use medication to solve all cases of azoospermia, but in some situations, the pathway for sperm to leave the body is blocked, or sperm production itself is significantly impaired. TESA, PESA, and TESE are designed to collect whatever sperm are present at the source, either in the epididymis or within the testicular tissue.
In 2026, they are part of a toolkit that also includes hormonal evaluation, genetic testing when indicated, and careful planning of IVF or ICSI cycles. We use these tools in combination rather than relying on a single solution.
TESA (Testicular Sperm Aspiration): How It Fits Into IVF And ICSI
TESA focuses on aspirating testicular tissue and fluid through a fine needle, typically under local or light general anesthesia. The laboratory team then processes this tissue, looking carefully for viable sperm that can be used that same day or frozen for future treatment.
Clinically, TESA is often discussed with men who have non‑obstructive azoospermia, but it may also be used in some obstructive cases based on the urologist’s evaluation. Because TESA retrieves relatively small amounts of tissue, it is usually matched with ICSI, where only a small number of sperm may be required.
When We Consider TESA
We usually discuss TESA if semen samples show no sperm and there is concern that sperm production may be reduced but not absent. Hormone profiles, testicular size, and sometimes genetic findings help us decide if TESA is a reasonable option to explore.
We also consider whether this will be combined with fresh IVF and ICSI in the same cycle, or whether sperm will be retrieved and frozen first, then used in a later IVF cycle. The plan is highly individual and shaped by how comfortable you are with each step.
TESA And ICSI In Practice
Because TESA often yields small numbers of sperm, using it together with ICSI is common in male‑factor IVF cycles in 2026. The embryologist can choose individual sperm that look most promising, then inject them directly into each mature egg.
We never promise that a particular TESA attempt will provide usable sperm or lead to pregnancy, but we use published data and our own experience to explain likely ranges of retrieval rates and how that compares with other options such as donor sperm.
PESA (Percutaneous Epididymal Sperm Aspiration): A Key Option In Obstructive Azoospermia
PESA targets the epididymis, where sperm normally mature and are stored before ejaculation. In obstructive azoospermia, sperm production can be adequate, but a blockage in the ducts prevents sperm from appearing in the semen, so PESA aims to access stored sperm above the blockage.
Recent data show that percutaneous retrieval strategies that combine PESA and rescue TESA can achieve cumulative sperm retrieval rates reported at 100% in obstructive azoospermia cohorts, with reported pregnancy rates around one‑third at first retrieval and higher with repeats. These figures are study‑specific and not guarantees, but they explain why PESA remains central in obstructive cases in 2026.
How PESA Is Performed
PESA is a needle procedure through the skin of the scrotum into the epididymis, usually under local anesthesia. Fluid aspirated from the epididymis is immediately examined in the lab to look for motile sperm.
If enough sperm are present, some can be used fresh for ICSI and some can be frozen, depending on your plan. If no sperm are found, urologists may discuss proceeding to a testicular retrieval approach, such as rescue TESA, in the same session.
PESA Outcomes In Context
For obstructive azoospermia, percutaneous epididymal approaches are often considered first, because sperm quality may be closer to ejaculated sperm than in some testicular retrievals. However, outcomes still depend on individual anatomy and the precise cause of the blockage.
We explain that while studies report very high retrieval rates with combined percutaneous methods, each clinic’s experience and each patient’s situation are different. Our aim is to share numbers transparently without turning them into promises.
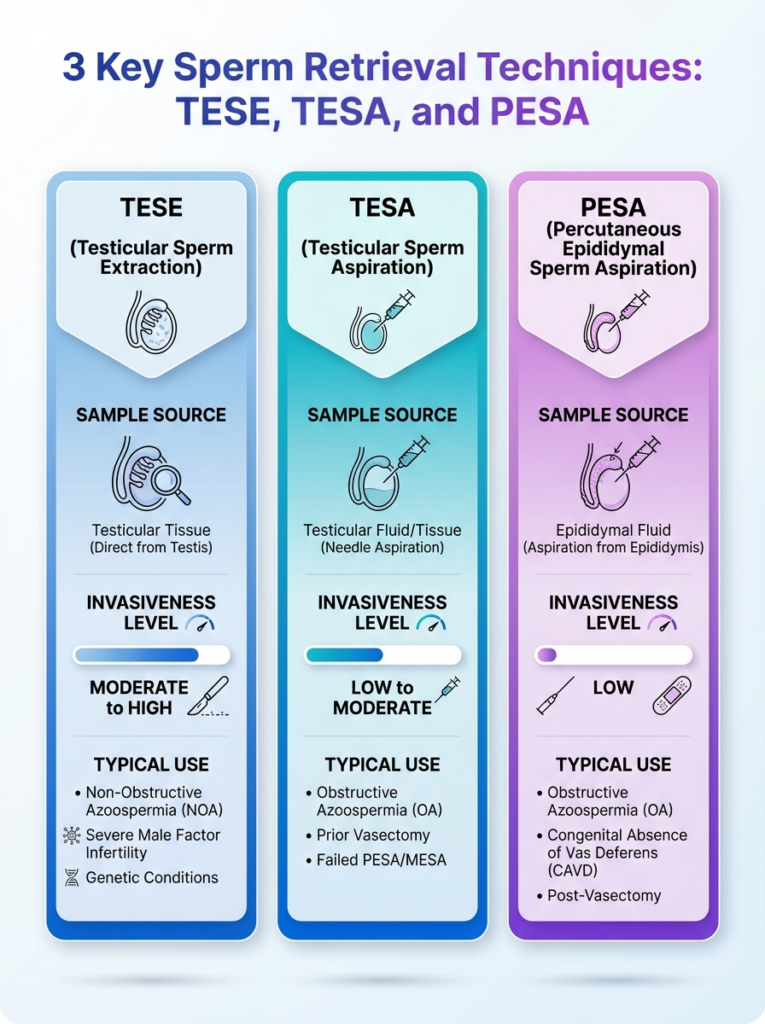
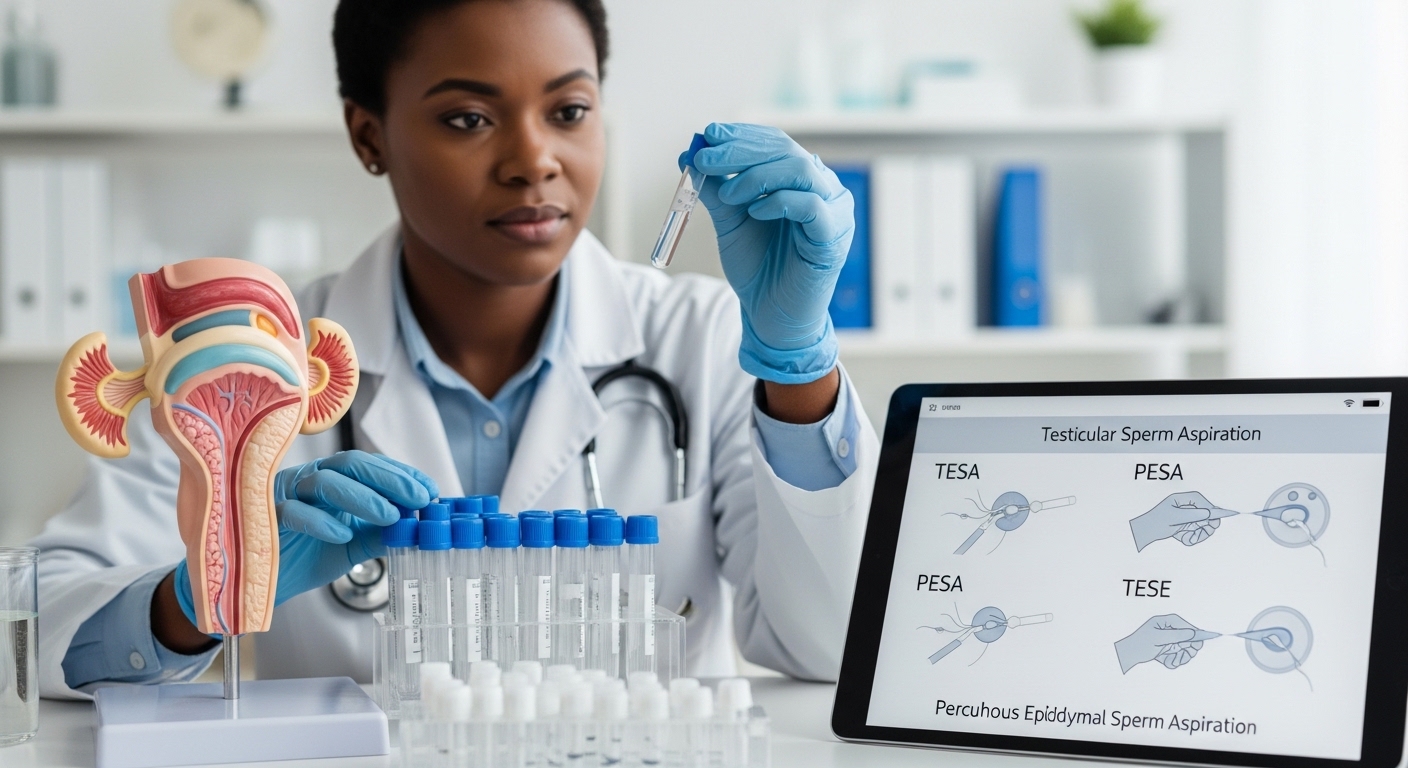
An at-a-glance guide to TESE, TESA, and PESA sperm retrieval techniques. Learn how each method is used in male fertility treatment.
TESE (Testicular Sperm Extraction): Classic And Micro‑Surgical Variants
TESE means surgically taking tiny pieces of testicular tissue and then searching for sperm under a microscope in the lab. In 2026, TESE can range from a simple open biopsy to more refined approaches, including micro‑TESE that use magnification to look for areas of active sperm production.
Multi‑center studies of idiopathic non‑obstructive azoospermia report micro‑TESE sperm retrieval rates slightly above 50%, with predictive models that consider hormone levels and testicular histology. Those figures help us counsel patients on probabilities, but they do not predict what will happen in any single operation.
Standard TESE Versus Micro‑TESE
Standard TESE involves removing small tissue fragments from one or both testes without high magnification, while micro‑TESE uses an operating microscope to identify the most promising tubules. Randomized data have suggested that loupe‑assisted TESE can have similar retrieval rates to full micro‑TESE in some NOA populations, with shorter operative times.
Choosing between these TESE variants is not a one‑size‑fits‑all decision. We consider the underlying diagnosis, prior surgeries, testicular volume, and your preferences regarding invasiveness and potential repeat procedures.
What TESE Means For Your IVF Plan
Because TESE is more invasive than needle aspiration, many couples prefer to combine the retrieval with sperm freezing, in case repeat procedures can be avoided. When sperm are found, the lab team usually prepares multiple vials for future ICSI cycles, which can be especially important if the underlying condition is stable.
If no sperm are retrieved, we talk through donor options and other pathways in a structured way. The key in 2026 is to plan TESE as part of a broader fertility roadmap rather than as a standalone event.
Did You Know?
Combining microTESE and trifocal TESE in nonobstructive azoospermia has been reported to yield around 63.4% sperm retrieval rates overall, with more cryopreserved vials per patient compared with using one technique alone.
How TESA, PESA, and TESE Integrate With IVF, ICSI, And ART Pathways
TESA, PESA, and TESE rarely stand on their own in 2026; they usually sit within a structured assisted reproductive technology pathway. Our IVF and ICSI plans are built around egg stimulation, egg retrieval, fertilization in the lab, embryo culture, and embryo transfer, and sperm retrieval procedures are coordinated to support those stages.
For many couples with severe male‑factor infertility, the most common combination is surgical sperm retrieval plus ICSI, sometimes with genetic testing of embryos when indicated. We discuss this whole journey in advance, so you know how the male and female procedures line up.

From Sperm Retrieval To Fertilisation
Once sperm are retrieved, our embryologists decide whether to use them fresh or thaw previously frozen samples, depending on timing. In ICSI cycles, a single sperm is selected for each egg, which means even very low sperm numbers can still be clinically useful.
In some mild male‑factor cases, retrieved sperm may be used with conventional IVF or even IUI, but this is less typical for azoospermia. We always clarify which method we are planning and why.
Role Of PGT And Other ART Techniques
Some couples also consider preimplantation genetic testing of embryos, especially if there are known genetic risk factors or recurrent miscarriage. While PGT focuses on embryo chromosomes rather than sperm retrieval success, it can be relevant in planning how many eggs to fertilise and transfer.
We explain how TESA, PESA, TESE, ICSI, and PGT can be combined in a sequence that suits your diagnosis and values. The goal is to provide information that is realistic and specific, not generic promises.
Comparing TESA, PESA, TESE: Techniques, Use Cases, And Practical Differences
Couples often ask us for a side‑by‑side comparison of TESA, PESA, and TESE, so they can see in simple terms how these techniques differ. While each case is unique, some recurring patterns in 2026 help shape expectations.
The table below highlights typical features and typical use‑cases, without claiming that one technique is universally better than another.
| Technique | Target Area | Typical Use | Procedure Style |
|---|---|---|---|
| PESA | Epididymis | Obstructive azoospermia with suspected normal production | Percutaneous needle aspiration under local anesthesia |
| TESA | Testicular tissue | Obstructive or non‑obstructive cases where epididymal access is not suitable | Needle aspiration of testicular tissue, usually day procedure |
| TESE | Testicular tissue | Non‑obstructive azoospermia, especially complex or previous failures | Surgical extraction of small tissue fragments, standard or micro‑surgical |
Importantly, the decision between these options is not made in isolation. We work with urologists, reproductive endocrinologists, and embryologists to tailor the technique based on your diagnosis and prior history.
We also discuss how many attempts you feel comfortable considering, especially because repeated micro‑TESE tends to show lower sperm retrieval rates than first‑time procedures in published data.
Success Rates, Limitations, And What Statistics Really Mean For You
In 2026, couples have access to more published sperm retrieval data than ever before, but interpreting those numbers can be challenging. We see figures for micro‑TESE, combined TESE strategies, and percutaneous approaches such as PESA with rescue TESA, yet every figure is tied to a specific study design and patient group.
When we discuss these numbers, we treat them as evidence to inform expectations, not as guarantees of a specific outcome. Individual factors like testicular histology, hormone levels, age, and underlying diagnoses play crucial roles in actual retrieval possibilities.
Did You Know?
In some analyses of nonobstructive azoospermia, sperm donation was used in about 12.66% of assisted reproduction cycles overall, with different utilization patterns depending on whether sperm were retrieved via microTESE or TESA.
What Retrieval Statistics Can And Cannot Say
Retrieval percentages describe how often sperm were found in a study population, not how often pregnancy or live birth occurred. They also cannot predict in advance which individual patient will fall into which category.
We use them to answer questions such as whether a repeat micro‑TESE is reasonable, or whether a move to donor sperm may be more likely after prior failed attempts. Your comfort level with uncertainty is part of this conversation.
Balancing Hope With Realism
We are careful not to promise that any TESA, PESA, or TESE attempt will provide sperm or lead to pregnancy, even when studies report encouraging numbers. At the same time, we want you to see that many couples do proceed with these procedures as part of evidence‑based care.
Our role is to provide accurate information, explain how we apply it in clinical decisions, and help you choose a path that respects both your goals and your tolerance for risk and intervention.
Planning Your Journey: From Diagnosis To Sperm Retrieval Decision
Before considering TESA, PESA, or TESE, we start with a thorough evaluation of male fertility, including semen analysis, hormonal tests, and selected imaging or genetic investigations. This groundwork helps us distinguish obstructive from non‑obstructive azoospermia and identify any broader health issues that may need attention.
Once we have a clearer diagnosis, we discuss the likely pros and cons of each retrieval approach, how they align with your IVF or ICSI plans, and what timelines are realistic. Our aim is for you to feel prepared rather than rushed when making decisions about surgery.
- Confirm whether azoospermia is obstructive or non‑obstructive.
- Review hormone levels and overall reproductive history.
- Discuss potential retrieval techniques and possible outcomes.
- Align retrieval timing with egg collection and embryology planning.
This planning phase is also when we talk about options if retrieval does not find sperm, so you are not forced into big decisions under time pressure. Having contingencies in place often reduces anxiety for both partners.
When Sperm Retrieval Is Not Enough: Donor Sperm, Donor Embryos, And Other Paths
Even with modern TESA, PESA, and TESE strategies, some couples discover that no usable sperm can be obtained. In those situations, donor sperm or donor embryos may provide alternative paths to parenthood, and we discuss them carefully and respectfully.
Choosing to move toward donor options is highly personal and can involve a period of reflection, counseling, and further questions about genetics, identity, and family planning. We encourage you to explore these topics at your own pace, without pressure.
- Sperm donation: Using screened donor sperm in IUI or IVF cycles.
- Donor embryo programs: Adopting embryos that have been created by other patients.
- Egg donation: Sometimes relevant when both male and female factors exist.
For some couples, simply knowing that donor paths exist brings a sense of relief during the sperm retrieval decision process. It means that even if TESA, PESA, or TESE do not lead to usable sperm, other routes can still be explored.
Emotional And Practical Support During TESA, PESA, TESE Treatment
Medical details are only part of the story, because even the idea of testicular or epididymal procedures can feel confronting. In 2026, we see many couples benefit from psychological support, peer groups, or simply having more structured information about each step.
We encourage open conversations between partners about expectations, fears, and boundaries around surgery, donor options, and the number of attempts you wish to consider. Clear communication can reduce misunderstandings and support joint decision‑making.
Tip: Many couples find it helpful to write down their questions about TESA, PESA, TESE before appointments, so they leave with clear answers rather than lingering doubts.
On the practical side, we walk you through logistics such as time off work, support at home after recovery, and coordination with the female partner’s treatment. Good planning can make the clinical experience feel more manageable.
Conclusion
In 2026, TESA, PESA, and TESE give many couples a structured way to explore sperm retrieval when semen samples show no sperm or very low counts. These techniques are not guarantees and they are not the right choice for everyone, but they sit at the heart of modern care for male‑factor infertility when used thoughtfully within an IVF and ICSI pathway.
Our commitment is to explain each procedure clearly, share what current research suggests without overstating its meaning, and help you map out a realistic plan that fits your medical situation and personal values. Whether you proceed with TESA, PESA, TESE, or choose a different route such as donor options, we are here to help you navigate the choices with honest, grounded information.

