
Controlled ovarian stimulation for IVF often means 9 to 12 days of injections, and in a large 2024 trial, the average stimulation length was 9.2 days with certain protocols versus 12.1 days with others, so understanding your induction plan and schedule in advance can sharply change how this phase feels. In 2026, we see more patients asking not only “Will IVF work?” but “Exactly what medications, on which days, and why?”
Key Takeaways
| Common Question | Concise Answer |
|---|---|
| 1. What is an IVF induction protocol in 2026? | It is the structured plan your clinic uses to stimulate your ovaries, prevent premature ovulation, and time egg retrieval, using specific medications on specific days. You can see how this fits into the full IVF journey in our guide Infertility and IVF explained. |
| 2. Which stimulation protocol is “best” for IVF? | Evidence suggests several protocols can be effective, and the “best” choice depends on factors like age, ovarian reserve, PCOS, and risk of ovarian hyperstimulation syndrome, which we discuss further in our factors affecting IVF success rate guide. |
| 3. How long do IVF stimulation injections usually last? | Most cycles involve around 8 to 12 days of stimulation before trigger, although individual plans vary. Our category hub for IVF articles explores how protocol choice and age influence this. |
| 4. How do protocols relate to IVF success rates? | Studies show both GnRH agonist and antagonist approaches can support pregnancies, and success also depends on embryo quality, embryo transfer strategy, and overall health, topics we expand on in our IVF success strategies guide. |
| 5. How does induction differ for PCOS or secondary infertility? | Patients with PCOS or secondary infertility may need tailored dosing and protocol types to balance egg yield and safety, and we encourage reading our resources on PCOS and secondary infertility when preparing for consultation. |
| 6. Where can I explore broader fertility health before IVF? | Our fertility hub and reproductive health collection cover lifestyle, ovulation, and clinic choice, all of which sit alongside your medication schedule. |
| 7. How do I cope with daily injections and timing? | Clear written plans, reminders, and supportive education can help, and our broader health and wellness articles offer stress and routine tips that many IVF patients use during induction. |
1. IVF Induction Protocols 101: What “Stimulation” Really Means
When we talk about IVF induction in 2026, we are talking about controlled ovarian stimulation, where we use medications to help you grow multiple follicles in a single cycle. The goal is to collect several mature eggs in a carefully timed egg retrieval, not to alter your fertility permanently.
Every protocol pairs three building blocks: stimulation drugs that encourage follicle growth, suppression drugs that keep you from ovulating too early, and a timed trigger shot that readies eggs for retrieval. Your protocol, dose, and schedule are personalised, so two patients rarely have identical calendars even if they use similar medications.

2. Core IVF Stimulation Medications And What They Do
Most induction schedules revolve around injectable gonadotropins, laboratory-formulated versions of FSH or a mix of FSH and LH. These are the medications you give yourself daily in your lower abdomen using fine needles, typically starting on day 2 or 3 of your menstrual cycle.
To keep follicles from releasing eggs too early, clinics add either GnRH antagonists, GnRH agonists, or in some newer approaches, oral progestins. Despite different names, these drugs share one goal, which is keeping ovulation “on hold” until we deliberately trigger it.
How We Explain Medicines To Our Patients
In our consultations, we group medications into three simple categories: “grow”, “hold”, and “release”. Growth drugs are your daily stimulation injections, hold drugs are your suppression medications, and the release drug is your trigger shot.
Using this language can make a crowded schedule less overwhelming, and it often helps partners follow along with what each injection is doing in real time.
3. GnRH Antagonist Protocols: Shorter, Flexible Induction Cycles
GnRH antagonist protocols are widely used in 2026 as a first-line option for many IVF patients, because they fit into shorter and often more flexible schedules. In a large multicenter IVF trial, antagonist cycles averaged about 9.2 days of stimulation compared with 12.1 days for some long agonist cycles, which means fewer injection days for many patients.
In this approach, you start your daily FSH or FSH/LH injections first, then add a GnRH antagonist partway through, usually around stimulation day 5 or when leading follicles reach a certain size. The antagonist is continued daily or almost daily until your trigger shot, after which egg retrieval is scheduled down to the hour.
Ready To Start Your IVF Journey?
Speak with our fertility specialists about the right IVF induction protocol, medication schedule, and treatment plan tailored to your needs.
Book A ConsultationWhy Many Clinics Use Antagonists For High‑Risk Patients
Guidance documents suggest that GnRH antagonist protocols can lower the risk of ovarian hyperstimulation syndrome compared with some long GnRH agonist approaches, especially in patients who are prone to very high egg yields such as some women with PCOS. For patients, this can translate into a safety discussion at the very beginning of IVF planning.
Because antagonist cycles tend to be shorter and less suppressive overall, many patients report that they feel closer to a “natural” cycle even though induction still involves daily injections and close monitoring.
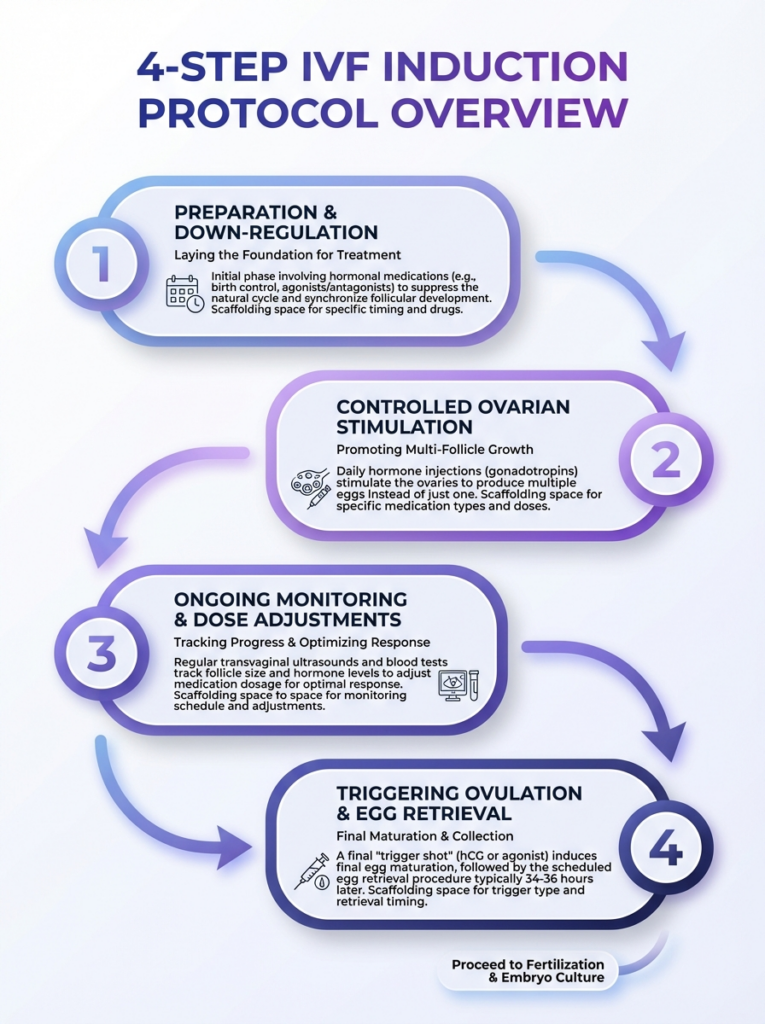
A concise 4-step overview of IVF induction protocols and medication timing. This infographic clarifies schedules and medications used during the induction phase.
4. Long GnRH Agonist Protocols: Structured Suppression For Selected Patients
In a long GnRH agonist protocol, we first use a GnRH agonist to temporarily quiet your own hormonal cycle before starting high-dose stimulation. In most calendars, this means beginning a nasal spray or daily agonist injection in the cycle before stimulation, then adding FSH after a bleed or a set number of days.
Some large analyses have suggested that long GnRH agonist protocols may be associated with higher cumulative live birth rates across a complete stimulated cycle in certain groups, although results differ between studies and populations. Because we must not overstate results, it is important to treat these figures as signals to discuss with your specialist rather than guarantees.
Have Questions About IVF Medications?
Chat directly with our team for guidance on IVF induction schedules, injections, fertility consultations, and treatment options.
Chat On WhatsAppAgonist Versus Antagonist: How We Frame The Conversation
When we compare protocols with our patients, we focus on practical differences such as calendar length, injection burden, and individual risk factors rather than promising that one protocol will outperform another for every person. Meta-analyses have reported broadly comparable live birth rates between long agonist and antagonist protocols, with a safety advantage for antagonists in some settings.
Your doctor will also consider special situations such as endometriosis, repeat implantation failure, or the need for precise calendar control when proposing an agonist-based induction.


Did You Know?
Across meta-analyses, GnRH antagonist protocols show comparable live birth rates to long GnRH agonist protocols while consistently reducing ovarian hyperstimulation syndrome risk, which is why many clinics in 2026 consider antagonists a safe, effective first-line option for a wide range of patients.
5. Progestin‑Primed Ovarian Stimulation (PPOS) And Other Emerging Options
Progestin‑primed ovarian stimulation, often called PPOS, uses an oral progestin alongside daily gonadotropins to prevent premature LH surges instead of a GnRH analog injection. In recent research, PPOS with dydrogesterone suppression yielded similar clinical pregnancy outcomes to standard antagonist protocols while producing higher numbers of retrieved and mature oocytes and promising embryo quality in some cohorts.
Because PPOS typically requires freezing all embryos rather than fresh transfer, it sits mainly in the toolkit of clinics that already have strong vitrification and frozen transfer programs. In 2026, this approach is often discussed with patients who value fewer injections or whose clinics are planning frozen embryo transfer for other reasons.
Who Might Hear About PPOS In Consultation
PPOS conversations tend to arise for patients undergoing elective fertility preservation, such as oocyte or embryo freezing, or when we are building a strategy of “stimulate now, transfer later”. The decision to use PPOS also depends on available medications, regulatory environment, and laboratory strategy.
Because these protocols are newer, we emphasise that long term comparative data are still growing, and that progestin priming is one among several valid suppression strategies rather than a universal upgrade.
6. Typical Day‑By‑Day IVF Medication Schedule: A Sample Calendar
Although your personalised calendar will differ, it is helpful to see a high-level example of how a standard antagonist induction schedule might look in 2026. The table below is an illustrative overview, not a prescription, and your clinic will adapt timing, drugs, and doses to you.
| Cycle Day | Typical Medications | Monitoring |
|---|---|---|
| Day 1 | Period starts, confirm with clinic | Baseline blood tests and ultrasound may be scheduled |
| Day 2–3 | Start daily FSH or FSH/LH injections | Baseline scan and hormone panel if not done Day 1 |
| Day 5–6 | Continue stimulation, add GnRH antagonist once follicles reach target size | First response scan and blood tests |
| Day 7–10 | Daily FSH and antagonist, dose adjustments as needed | Regular ultrasounds and hormones to guide timing |
| Trigger day | Stop antagonist, give hCG or GnRH agonist trigger at set time | Final scan earlier that day to confirm readiness |
| 36 hours later | Egg retrieval under sedation | Recovery monitoring and post‑op instructions |
Other protocols, such as long agonist or PPOS, reposition suppression drugs to earlier in the cycle or into the luteal phase before stimulation, so the exact “Day 1” of injections can vary. We always pair calendars like this with written instructions and in-person teaching so you can double check each step.
7. Safety, OHSS Risk, And Why Protocol Choice Matters
Safety is one of the first reasons we choose a stimulation protocol and schedule in 2026, particularly regarding ovarian hyperstimulation syndrome. OHSS is a response where ovaries become very enlarged and fluid can shift in the body, and protocol type, trigger medication, and embryo transfer strategy all play roles in how often it appears.
Guideline documents and meta‑analyses report that GnRH antagonist cycles tend to show lower rates of OHSS compared with many long GnRH agonist cycles, while maintaining comparable live birth rates in most studied populations. High‑risk groups such as patients with PCOS have seen meaningful relative risk reductions for OHSS when antagonists are used in stimulation.
Using Trigger Type And Freeze‑All Strategies Thoughtfully
Beyond protocol choice, modern IVF in 2026 often adds a GnRH agonist trigger and freeze‑all approach to further limit OHSS risk in very responsive ovaries. This means we still stimulate the ovaries but decide in advance not to perform a fresh transfer if risk markers are high.
We discuss these options clearly during planning since they change not just your induction medications but also when you might be able to try embryo transfer.
Did You Know?
In a large randomized trial, severe ovarian hyperstimulation syndrome occurred in about 5.1% of GnRH antagonist cycles compared with 8.9% of long-acting GnRH agonist cycles, with moderate OHSS 10.2% vs 15.6% respectively, which highlights why antagonists are often chosen for patients at higher risk in 2026.
8. Tailoring Induction Protocols For PCOS, Endometriosis, And Secondary Infertility
Not every ovary behaves the same way, and we adjust induction schedules accordingly for PCOS, endometriosis, and secondary infertility in 2026. Patients with PCOS often have a high follicle count at baseline, so we may start at lower doses, monitor more closely, and lean toward antagonist or modified protocols that give us more flexibility to control response.
For women with endometriosis, research has reported that both agonist and antagonist protocols can achieve comparable pregnancy outcomes, while antagonists may offer a safety advantage in some scenarios. In secondary infertility, age at current treatment, time since last pregnancy, and any new diagnoses all feed into protocol choice.
Why Your Previous Cycles Matter
If you have undergone prior ovulation induction, IUI, or IVF cycles, we look closely at how your ovaries responded to previous medications before designing a new schedule. This might mean changing drug brands, changing from agonist to antagonist, or adjusting the start day of suppression medications.
Our aim is to learn from every prior stimulation, whether it was part of a simple fertility treatment or a full IVF cycle, and make your 2026 protocol as informed and personalised as possible.
9. Medication Adherence, Injection Anxiety, And Real‑World Challenges
Perfect protocols on paper still rely on real people giving themselves injections at the right dose and time, often while working or caring for families. A real‑world French study reported that roughly 27 percent of patients self‑reported noncompliance with their ovarian stimulation injections, and around one third felt anxious about self‑injection, with over 20 percent showing discrepancies between what they remembered and what physicians recorded.
These figures underline why, in 2026, we place so much emphasis on simple written plans, reminder systems, and in‑person teaching before your first injection. We also encourage partners or trusted friends to attend injection training so that you do not feel alone in managing the schedule.
Practical Tips We Share For Staying On Schedule
- Keep a printed calendar on your fridge and a duplicate on your phone.
- Set at least two alarms for daily injections, ideally at the same time each evening.
- Use a small tray or basket to hold all current‑cycle medications so you do not misplace pens or vials.
- Call your clinic immediately if you miss or double a dose so they can advise next steps.
We also point patients to supportive wellness resources, since managing stress and sleep often makes handling a complex medication schedule feel more manageable.
10. From Trigger To Transfer: What Happens After Induction Ends
Once stimulation and suppression phases are complete and we schedule your trigger shot, your induction protocol moves into its final timed steps. The trigger is usually given about 36 hours before egg retrieval and is very time sensitive, which is why clinics stress precise injection timing on that evening.
After retrieval, your induction phase is over, but your medication schedule continues into the luteal phase with progesterone and sometimes other supports. In antagonist cycles, some newer research has explored adding small GnRH agonist doses during the luteal phase, with one 2025 study reporting higher clinical pregnancy rates in cycles that used agonist‑supplemented luteal support compared with standard support alone.
Connecting Induction Choices To Embryo Transfer Strategy
Induction protocols do not stand alone, and their effects ripple forward into embryo management. For example, in antagonist cycles with only a few high‑quality Day 3 embryos, one large dataset suggested that immediate Day 3 transfer achieved higher cumulative live birth rates than extending all embryos to blastocyst, which can influence how we design the overall plan.
When we design your induction protocol in 2026, we already have a working idea of what we will do if you have many embryos, few embryos, or need to delay transfer, so that your schedule and expectations stay aligned from start to finish.
Have Questions About IVF Medications?
Chat directly with our team for guidance on IVF induction schedules, injections, fertility consultations, and treatment options.
Chat On WhatsAppConclusion
In 2026, IVF induction protocols and medication schedules combine established evidence with genuine personalisation, which is why two patients can be on IVF yet follow very different calendars. Antagonist, agonist, and progestin‑primed strategies can all support effective ovarian stimulation, but each carries distinct implications for safety, convenience, and embryo planning.
Our role is to translate these options into clear, actionable schedules you can follow with confidence, supported by written plans, teaching, and ongoing dialogue. If you are preparing for IVF now, bringing questions about protocols, trigger timing, and daily routines to your next consultation is one of the most powerful ways to shape a plan that fits both your body and your life.

